When Depression Takes Over, Therapy Can Help You Find Your Way Back
Depression therapy is a broad term for the professional treatments used to reduce symptoms of major depressive disorder and help people rebuild their daily lives. If you’re trying to understand your options, here’s a quick overview:
Main depression therapy options:
- Cognitive Behavioral Therapy (CBT) — changes negative thought and behavior patterns; 6–20 weekly sessions
- Interpersonal Psychotherapy (IPT) — focuses on relationship problems and life transitions; 16–20 sessions
- Mindfulness-Based Cognitive Therapy (MBCT) — combines mindfulness and cognitive skills; best for relapse prevention
- Behavioral Therapy — increases positive activities to lift mood; 20–24 sessions
- Antidepressant Medication — SSRIs, SNRIs, and NDRIs; often combined with therapy for better results
- Advanced options — TMS, ECT, or ketamine for treatment-resistant cases
Depression is one of the most common mental health conditions in the world, affecting roughly 9% of U.S. adults in any given year. Yet many people struggle for months — or years — before finding a treatment that actually works.
The hard truth? Traditional antidepressants alone relieve symptoms in only about one-third of patients. That means for most people, medication by itself isn’t enough.
The good news is that there are multiple evidence-based therapies — and research consistently shows that combining psychotherapy with the right support leads to better, longer-lasting outcomes.
Whether you’re newly diagnosed, frustrated by treatments that haven’t worked, or simply trying to understand your options, this guide breaks down what the research actually says — in plain language.

Evidence-Based Psychotherapy Options for Adult Depression
When it comes to treating major depressive disorder in adults, talk therapy is far more than just “venting” to a sympathetic listener. Modern psychotherapy is a structured, evidence-based medical intervention. According to the APA guidelines on adult depression treatments, there are several highly effective therapeutic models designed to target the specific cognitive, behavioral, and relational patterns that keep us stuck in a depressive episode.
The typical session structure for these therapies involves meeting once a week for 50 to 60 minutes. Depending on the modality, treatment duration can range from short-term interventions (lasting 6 to 20 weeks) to longer-term structural work. Understanding how these approaches differ is the first step in navigating therapy options without losing your mind.
Cognitive Behavioral Therapy (CBT) as a First-Line Depression Therapy
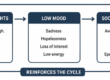
Cognitive Behavioral Therapy (CBT) is widely considered the gold standard of depression therapy. It operates on a simple, powerful premise: our thoughts, feelings, and behaviors are deeply interconnected. When we are depressed, our brain gets trapped in a negative feedback loop. A negative thought leads to a painful emotion, which leads to behavioral withdrawal, which in turn reinforces the negative thought.
CBT breaks this cycle using two primary engines: cognitive restructuring and behavioral activation.
- Cognitive Restructuring: Therapists help you identify “automatic thoughts”—those immediate, often irrational criticisms that pop into your head (e.g., “I ruin everything”). By using thought records, you learn to write down these thoughts, analyze the actual evidence for and against them, and replace them with realistic, balanced perspectives.
- Socratic Questioning: Instead of simply telling you that your thoughts are incorrect, your therapist will ask targeted questions to help you discover cognitive distortions on your own.
- Behavioral Activation: This involves identifying activities that once brought you joy or a sense of accomplishment and scheduling them back into your life, even when your motivation is at zero.
The clinical evidence supporting CBT is massive. In a landmark CBT meta-analysis including 409 trials with 52,702 patients, CBT demonstrated moderate to large treatment effects compared to control conditions. Interestingly, while its short-term effects are comparable to medication, the research showed that CBT’s effects were significantly larger at 6-to-12-month follow-ups, proving that CBT teaches long-term coping skills that protect against future episodes. Overall, CBT boasts response rates ranging from 61% to 87% for depression treatment.
Behavioral Therapy vs. Cognitive Therapy
While CBT combines both elements, some therapists choose to focus primarily on one side of the coin. Understanding the difference between pure behavioral therapy and pure cognitive therapy helps clarify how therapists target different entry points of depression.
- Behavioral Therapy: This approach focuses almost entirely on behavioral activation and mood monitoring. The theory is that depression is maintained by a lack of positive reinforcement from our environment. When we feel down, we withdraw from social lives, stop exercising, and neglect hobbies. Behavioral therapy uses structured logs to track daily activities and mood, systematically scheduling pleasurable or productive tasks to reverse this downward spiral. It typically takes 20 to 24 weekly sessions.
- Cognitive Therapy: This approach focuses on the mind, specifically targeting negative schemas—deeply ingrained, early-learned beliefs about ourselves, the world, and the future (e.g., “I am fundamentally unlovable”). Cognitive therapy helps patients identify cognitive distortions (like all-or-nothing thinking or catastrophizing) and systematically challenge them over 8 to 28 weekly sessions.
Interpersonal Psychotherapy (IPT) for Relationship-Driven Depression
If CBT is about your relationship with your thoughts, Interpersonal Psychotherapy (IPT) is about your relationship with other people. IPT is a highly structured, time-limited treatment (usually 16 to 20 sessions) that views depression as a medical illness highly influenced by interpersonal interactions.
An IPT therapist will help you identify which of four primary “problem areas” is triggering or worsening your depression:
- Grief: Resolving complicated or delayed grief after the death of a loved one.
- Role Disputes: Navigating ongoing conflicts with a partner, family member, or co-worker.
- Role Transitions: Adjusting to major life changes, such as retirement, divorce, moving to a new city, or becoming a parent.
- Interpersonal Deficits: Addressing long-standing patterns of social isolation or difficulty forming meaningful relationships.
By focusing on improving communication skills, building a stronger social support network, and resolving these relational issues, IPT helps lift the heavy weight of depression.
Mindfulness-Based Cognitive Therapy (MBCT) for Relapse Prevention
For individuals who have experienced multiple major depressive episodes, the risk of relapse is incredibly high. Mindfulness-Based Cognitive Therapy (MBCT) was specifically designed to address this. Delivered in an eight-week group format (consisting of weekly two-hour sessions and a one-day retreat), MBCT blends the practical tools of cognitive therapy with mindfulness meditation.
Depression has a nasty habit of leaving “neural scars.” Even after recovering, a brief moment of sadness can trigger a cascade of automatic negative thoughts. MBCT teaches you to recognize these intrusive thoughts as transient mental events rather than absolute facts. By practicing body scans, mindful breathing, and non-judgmental awareness, you learn to step back from the cognitive patterns that lead to relapse, creating a buffer of mental resilience.
The Role of Medication and Combined Depression Therapy
While talk therapy is incredibly powerful, moderate to severe depression often benefits from a multi-front approach. This is where medical management enters the picture.
According to the Mayo Clinic guide on depression diagnosis and treatment, the decision to use medication should be made in consultation with a qualified medical professional, keeping in mind that a holistic approach to depression management often yields the most sustainable results.
Understanding Second-Generation Antidepressants
Second-generation antidepressants are the most commonly prescribed psychiatric medications today because they are generally safer and cause fewer side effects than older classes of drugs (like tricyclics or MAOIs). These medications target neurotransmitters—chemical messengers in the brain that regulate mood, sleep, and appetite:
- Selective Serotonin Reuptake Inhibitors (SSRIs): Drugs like escitalopram, sertraline, and fluoxetine prevent the reabsorption of serotonin, leaving more of this “feel-good” chemical available in the brain.
- Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs): Medications like duloxetine and venlafaxine boost both serotonin and norepinephrine, which can be particularly helpful for patients experiencing physical pain or severe fatigue alongside depression.
- Norepinephrine-Dopamine Reuptake Inhibitors (NDRIs): Bupropion is a common NDRI that targets norepinephrine and dopamine. Because it does not directly affect serotonin, it rarely causes the sexual side effects or weight gain common with SSRIs.
Comparing and Combining Medication with Depression Therapy
Is it better to do talk therapy or take a pill? The scientific consensus points to a clear winner: combined treatment.
While antidepressants can help lift the neurological “fog” of depression, they do not teach you how to manage stress, resolve relationship conflicts, or challenge negative thinking patterns. Conversely, severe depression can make it incredibly difficult to engage in the homework and cognitive tasks required in therapy. When used together, medication and psychotherapy have synergistic effects—the medication stabilizes your brain chemistry so you can actively participate in therapy, while therapy teaches you the skills needed to eventually taper off medication safely.
| Treatment Type | Average Response Rate | Major Advantages | Key Limitations / Drawbacks |
|---|---|---|---|
| Psychotherapy Alone (CBT) | 61% – 87% | No medical side effects; teaches long-term coping skills; lower relapse rates. | Requires active emotional effort; takes several weeks to show behavioral results. |
| Medication Alone (SSRIs/SNRIs) | ~33% (first try) | Relatively easy to adhere to; can quickly reduce severe physical/somatic symptoms. | Side effects (nausea, fatigue, sexual dysfunction); high relapse rates if stopped; does not teach coping skills. |
| Combined Treatment | Significant boost over monotherapy | Highest overall success rate; medication enables better engagement in therapy. | Higher overall cost; managing both medication side effects and therapy schedules. |
Advanced and Alternative Treatment Options
What happens when traditional antidepressants and standard talk therapies aren’t enough? Approximately 30% of people diagnosed with major depressive disorder experience treatment-resistant depression, meaning their symptoms persist even after trying multiple antidepressant classes. Fortunately, medical science in May 2026 offers highly effective, advanced treatments that target the brain directly.
- Repetitive Transcranial Magnetic Stimulation (rTMS): This FDA-approved, non-invasive procedure uses magnetic fields to stimulate nerve cells in the prefrontal cortex—the area of the brain involved in mood control. Standard rTMS improves symptoms in about 50% of patients, with over 30% achieving complete remission. Remarkably, when combined with psychotherapy, rTMS response and remission rates jump to 66% and 55%, respectively.
- The SAINT-iTBS Protocol: This is a cutting-edge, fMRI-guided accelerated TMS protocol. By using advanced neuroimaging to target the precise area of the brain unique to each patient, SAINT achieves a staggering 85.7% response rate and 78.6% remission rate in patients with treatment-resistant depression—often in just one week of intensive treatment.
- Electroconvulsive Therapy (ECT): Despite outdated Hollywood depictions, modern ECT is an incredibly safe, highly controlled medical procedure performed under general anesthesia. It remains one of the most effective treatments available, leading to rapid improvement in nearly 80% of patients, with 65% reaching remission within 4 weeks.
- Ketamine and Esketamine: Ketamine operates on glutamate pathways rather than traditional monoamines. It provides rapid, almost immediate symptom relief for about 60% of patients within 3 days of a single treatment, with 40% maintaining that response after one month.
- Light Therapy: Up to 90% of people with depression suffer from sleep issues, and about 40% of people with insomnia have clinical depression. For those with seasonal patterns, sitting in front of a specialized 10,000-lux light box for 30 minutes every morning improves symptoms in 50% to 60% of patients by regulating circadian rhythms. This is a wonderful, non-invasive tool to build into your resilience-building routines.
What to Consider When Choosing Your Treatment Path
Choosing how to address your depression is a highly personal decision. There is no “one-size-fits-all” cure. When weighing your options, keep these key factors in mind:
- Severity of Symptoms: Mild depression can often be resolved with lifestyle adjustments, self-help, or short-term counseling. Severe depression, especially when accompanied by suicidal ideation or an inability to perform basic self-care, usually requires a combination of medication and intensive therapy.
- Personal Preferences: Some people prefer the structured, homework-based approach of CBT, while others find healing in exploring relational dynamics through IPT.
- Side Effects and Risks: Antidepressants can cause physical side effects like dry mouth, weight gain, or sexual dysfunction. Additionally, the FDA requires a black box warning on all antidepressants regarding a slight increase in suicidal thoughts and behaviors in children, teens, and young adults under 25 during the first few weeks of treatment. Close clinical monitoring is essential.
- Co-occurring Conditions: If you struggle with trauma or anxiety alongside your low mood, your provider will need to adapt your care plan accordingly. Taking the time to understand the nuances of your condition is a vital step, which you can read more about in our comprehensive guide to understanding depression.
Compassionate Depression Counseling in Pennsylvania
At WPA Counseling, we understand that seeking help for depression can feel incredibly overwhelming. We are a compassionate group practice of licensed professional counselors based in Irwin, Pennsylvania, and we are dedicated to helping our neighbors throughout the state find their way back to joy and fulfillment.
Our Clinical Experience and Professional Background
Our team consists of highly trained, licensed professional counselors (LPCs) with deep clinical experience in treating major depressive disorder, persistent depressive disorder, and co-occurring anxiety or trauma. We don’t believe in clinical, cold, or sterile therapy. We bring our authentic, warm, and down-to-earth selves into every session, combining clinical expertise with genuine human connection.
Our Local Practice History in Pennsylvania
WPA Counseling’s local practice history is rooted in serving individuals, couples, and families in Irwin, Westmoreland County, and surrounding Pennsylvania communities. Over time, our practice has grown to include both in-person counseling and secure telehealth, allowing us to support clients across Western and Central Pennsylvania while maintaining a strong connection to the local communities we serve.
Serving Our Western and Central Pennsylvania Communities
We are proud of our deep roots in Pennsylvania. We provide in-person counseling at our comfortable, welcoming offices in Irwin, PA (located in Westmoreland County, right near North Huntingdon PA), as well as secure, HIPAA-compliant telehealth therapy across all of Pennsylvania—including Pittsburgh, Penn Hills, and the broader Western and Central PA regions.
Our Unique Four-Stage Healing Process
We don’t just treat symptoms; we walk with you through a structured, thoughtful journey toward lasting wellness. Our signature four-stage healing process is designed to address both the surface-level struggles and the deeper root causes of your depression through counseling-based strategies:
- Rapport: Building a safe, non-judgmental, and trusting therapeutic relationship where you feel truly heard and understood.
- Wound Exploration: Safely identifying and understanding the underlying pain, past traumas, or negative life experiences that triggered your depressive patterns.
- Toxin Removal: Gently identifying and letting go of unhelpful coping mechanisms, negative core beliefs, and toxic relational patterns through therapeutic reflection, skills practice, and healthier emotional regulation.
- Truth Restoration: Rebuilding your life on a foundation of authentic self-worth, healthy boundaries, and realistic, positive truths about who you are.
Whether you prefer sitting face-to-face in our cozy Irwin office or connecting from the comfort of your own home via online therapy, we adapt our approach to fit your lifestyle. You can learn more about how we are modernizing care in our article on why in-person depression counseling in PA is evolving.
Frequently Asked Questions About Depression Therapy
How long does depression therapy typically last?
Depression treatment is generally broken into phases. Acute treatment focuses on reducing active symptoms and usually lasts 6 to 20 weeks with a session frequency of once per week. Once you feel better, continuation treatment (typically lasting 4 to 9 months) helps consolidate your gains and prevent a immediate relapse. For those with chronic or recurrent depression, long-term maintenance therapy may continue on a bi-weekly or monthly basis.
What are the main risks or side effects of depression treatments?
While psychotherapy has no physical side effects, the process of emotional processing can temporarily increase emotional distress as you confront painful memories or difficult truths. Antidepressant medications carry risks of physical side effects (nausea, sleep issues, emotional numbing, sexual dysfunction) and physical dependence, meaning they must be tapered off gradually under a doctor’s supervision.
Is online depression therapy as effective as in-person counseling?
Yes! Extensive clinical research shows that telehealth is just as effective as in-person therapy for treating depression. Online therapy offers incredible accessibility, eliminating commute times and making it easier for busy professionals, parents, or those with mobility challenges to receive consistent care. If you are living in the Pittsburgh area, you can read our tips on how to find online depression therapy Pittsburgh residents trust.
Conclusion
Depression is a heavy, isolating burden, but you do not have to carry it alone. From evidence-based talk therapies like CBT and IPT to advanced neuroscientific treatments, there are more ways to heal today than ever before.
At WPA Counseling, our licensed counselors in Irwin, PA, are ready to guide you through our specialized four-stage healing process. Whether you join us in person or online, we are committed to helping you restore your truth and reclaim your life.
If you are ready to take the first step toward feeling like yourself again, get started with professional depression therapy today. We are here, and we are ready to help.
This article was researched with AI and heavily edited by Stephen Luther for accuracy and relevance.
Stephen Luther is the Executive Director and Founder of WPA Counseling. He holds a Master’s degree in Education from the University of Georgia and a Master’s degree in Marriage and Family Therapy from Duquesne University. He is a licensed professional counselor in Pennsylvania (LPC).
Since 1997, Steve has been helping children, adolescents, adults, couples, and families overcome emotional and relational challenges. He specializes in working with hurting families, including those with foster, adopted, or traumatized children. Steve uses Attachment-Based Therapy, client-centered therapy, and Therapeutic Parent Coaching to support healing and relationship restoration.
This guide is for educational and spiritual encouragement and is not a substitute for personalized professional counseling. If you are in crisis, please reach out for immediate help.
The Complete Guide to Cognitive Behavioral Therapy
• Social Anxiety Treatment in Pennsylvania